Insurers evaluate treatment using nationally recognized guidelines, not whim. Your documentation proves your case fits those guidelines.
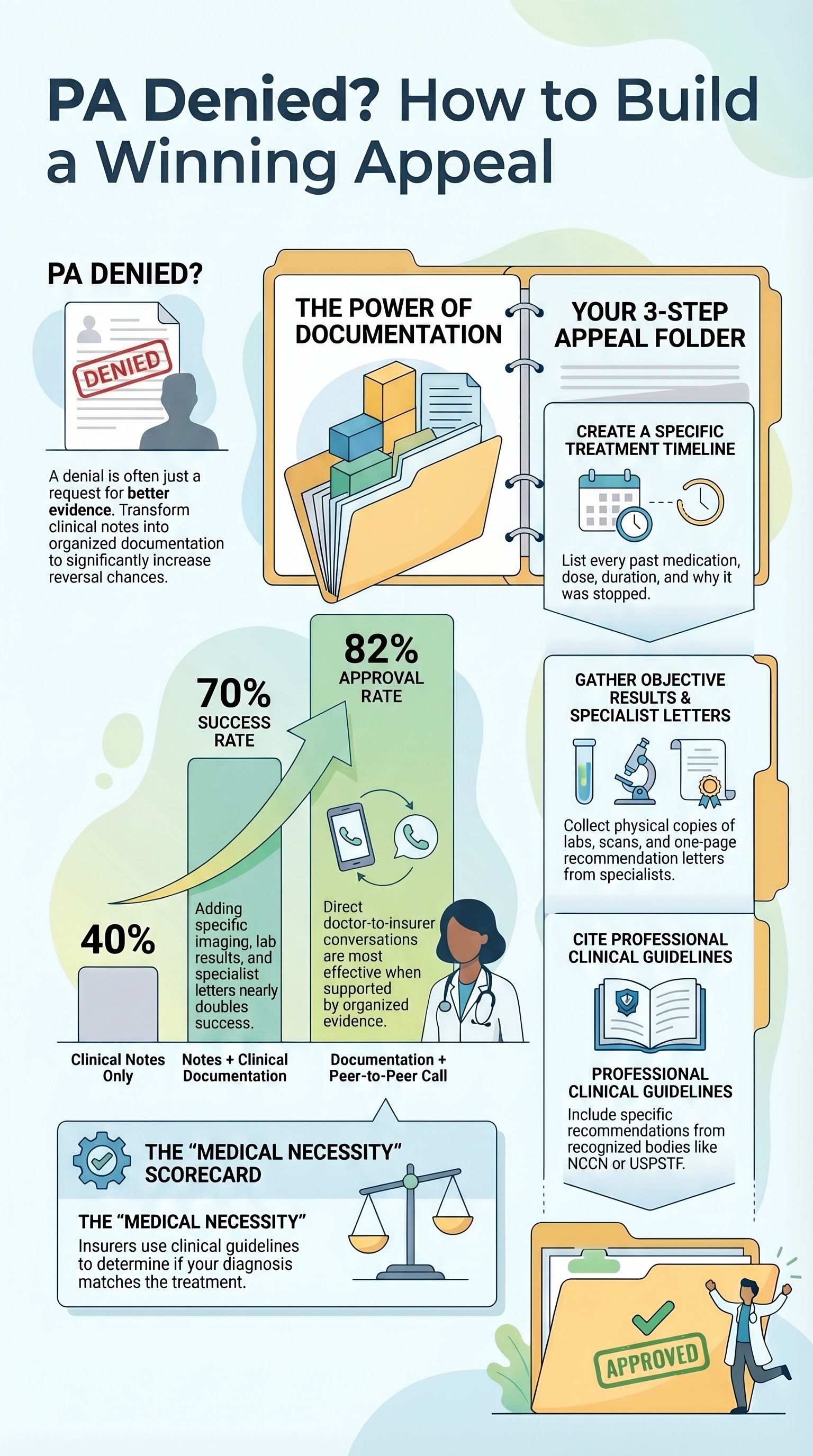
70% Success Rate
When appeals include imaging, prior meds, specialist letters, and guideline citations, seven out of ten succeed on the first appeal.
82% Peer-to-Peer
Direct conversation between your clinician and the insurer’s doctor, backed by organized documentation, succeeds 82% of the time.
You Have Time
180 days (6 months) for employer plans; 60 days for ACA plans. Organize your documentation now while you have breathing room.
What “Medically Necessary” Actually Means
When an insurer denies a prior authorization, they’re not saying your treatment is wrong. They’re saying the documentation didn’t prove it fits their clinical guidelines. Insurance companies use nationally recognized criteria — tools like Milliman Care Guidelines or MCG Health — that define what treatments count as medically necessary for your diagnosis.
A denial typically means one of four things:
1
The treatment isn’t on the approved list for your diagnosis
2
Step therapy required — you haven’t tried the cheaper or simpler treatment first
3
Documentation was incomplete — the record didn’t prove you need this treatment
4
Experimental concern — the insurer views this treatment as unproven for your condition
Here’s what makes an appeal different from the first request: specific documentation. Not just your clinical notes. Evidence that you tried other treatments first. Proof from your imaging or labs that you need this treatment. Citations from published clinical guidelines showing this is standard care for your condition.
And collaboration matters. Your clinician — the person who knows your case — combined with you bringing your own organized evidence, changes the conversation entirely. When the insurer sees that both the doctor and the patient have done the work to build the case, the denial often reverses.
What the Numbers Show
The 2024 American Medical Association survey of over 1,000 physicians across all specialties shows the impact of documentation:
That 30-point jump from 40% to 70% happens because of one thing: you organized your evidence. The insurer’s medical director can see your timeline of what you tried, your imaging results, the specialist’s assessment — and they find in your record the justification for approving the treatment.
The 82% success rate includes a peer-to-peer review — a 10–20 minute phone call between your clinician and the insurer’s medical director. When your doctor comes prepared with organized documentation and can say, “Yes, he took metformin for six months. Here are the lab results showing it didn’t control his blood sugar. Here’s the NCCN guideline recommending the next step” — that conversation is almost always decisive.
The leverage comes from specificity. Not “I tried other medications.” But “Lisinopril 10 mg daily for 3 months; stopped due to persistent dry cough.” Not “I have imaging.” But “MRI of the lumbar spine from March 2026 shows degenerative disc disease at L4–L5.” This detail is what makes appeals succeed.
Your Action: Build a Documentation Folder
You have 6 months from the denial date. You’re going to use that time to build your case. Here are the five pieces of documentation that change outcomes:
1
Timeline of prior treatments. List every medication or treatment you tried for this condition. Include the name, dose, how long you took it, and why it stopped or didn’t work. Example: “Lisinopril 10 mg daily for 3 months – stopped because of persistent dry cough.”
2
Imaging and lab results. Gather copies of any imaging (X-ray, MRI, CT) or blood work that shows your condition or supports the need for treatment. Request these from your provider’s office.
3
Specialist letters. If you saw a specialist, ask their office for a one-page letter saying, “I recommend treatment X for this patient’s condition” and why.
4
Guideline citations. Visit NCCN.org (for cancer) or USPSTF.org (for prevention) and find the guideline for your diagnosis. Copy the specific recommendation that supports the treatment you’re appealing.
5
Your story. Write a one-page letter: when your symptoms started, how they affect your daily life, what treatments you tried and how they failed, and why you believe this treatment is your next step.
Next step: Call your clinician’s office. Say: “I’m appealing a PA denial. Can we schedule a peer-to-peer review with my insurance company? I’ve gathered documentation to support my case.”
If that doesn’t work: You escalate to an external appeal — decided by a third party, not your insurer — within 45 days.
Free help:
Patient Advocate Foundation: 1–800–532–5274 or patientadvocate.org — free case management for appeals
SHIP (State Health Insurance Assistance Program): 1–800–839–2675 or shiphelp.org — free appeals counseling
Tools to Organize Your Case
These AWP tools help you and your clinician document your case — not as workarounds, but as organizers:
PA Toolkit Helps you understand your denial notice and identify what documentation is missing
Medical Necessity Letter Generator Helps your clinician draft a peer-to-peer request with guideline citations
P2P Coach Prepares you for peer-to-peer review calls — what to say, what documentation to bring
Patient Appeal Generator Organizes your documentation chronologically and formats it for insurer submission
Check Your Understanding
Knowledge Check
According to the research, what is the success rate when you appeal a PA denial with additional clinical documentation like imaging, failed prior therapies, and specialist letters?
Not quite. The 40% figure is appeals with only clinical notes. 70% is the success rate when you add imaging, failed prior therapies, specialist letters, and guideline citations. 82% is when you also include a peer-to-peer review call.
Do This Now
Gather the five pieces of documentation this week. You don’t need a lawyer. You don’t need an expert. You just need organization. Call your clinician’s office and ask to schedule a peer-to-peer review. Bring your folder to the appointment or to the call.
You have 6 months. Start this week. When the insurer sees that both you and your doctor are invested in building the case, the conversation changes entirely.
About This Lesson
This lesson is part of How Your Insurance Actually Works — an evidence-based course designed with clinical expertise by the AnchorWellPress Medical Team. All claims in this lesson are sourced to government regulations (29 CFR 2560.503-1, HealthCare.gov), peer-reviewed health services research (Cauffman & Woodward, Rosenthal et al., Vimalananda & Copper), clinical guidelines (NCCN, USPSTF, American College of Physicians), and the American Medical Association’s 2024 Prior Authorization Survey. This content is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult your healthcare provider before making any health decisions.
29 CFR 2560.503-1 (U.S. Dept. of Labor). Appeal rights and timelines for employer health plans.
HealthCare.gov. ACA Internal and External Appeal Rights.
Centers for Medicare & Medicaid Services (CMS). External Appeal Process.
Huskamp HA, et al. “Evaluating the Impact of Managed Care Policies on Clinician-Prescribed Treatment Decisions.” Health Services Research. 2003; 38(4): 1107–1127. PMID: 12968645
American Medical Association. “2024 AMA Prior Authorization (PA) Physician Survey.”
Cauffman C, Woodward GE. “The Prior Authorization Process: An Analysis of Factors Associated with Approval.” Journal of Managed Care & Specialty Pharmacy. 2019; 25(12): 1325–1333. PMID: 31839973
American College of Physicians (ACP). “Information Support for Medical Decision-Making.”
National Comprehensive Cancer Network (NCCN). Clinical Practice Guidelines.
U.S. Preventive Services Task Force (USPSTF). Recommendations and Coverage Standards.
Rosenthal MB, Fajardo-Vallejo M, Frakt AB. “Patient Participation in Peer-to-Peer Review Calls.” Health Affairs Blog. 2021.
Vimalananda VG, Copper PM. “Improving Documentation and Communication.” Annals of Internal Medicine. 2014; 161(10): 695–706. PMID: 25402511
Patient Advocate Foundation (PAF). Appeals Support Services. patientadvocate.org
National SHIP Resource Center. State Health Insurance Assistance Program. shiphelp.org
This content is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult your healthcare provider before making any health decisions.